
If you've been researching apheresis therapy and come across the term “inuspheresis,” you're not alone. It's generating significant interest online, particularly among patients exploring options for Long COVID, autoimmune conditions, and longevity medicine. This post explains what inuspheresis is, where it's available, and how it compares — technically and clinically — to therapeutic plasma exchange (TPE).
What Is Inuspheresis?
Inuspheresis is a proprietary form of double filtration plasmapheresis (DFPP), developed in Germany and Switzerland. Like TPE, it is an extracorporeal blood purification procedure, meaning blood is drawn from the patient, processed outside the body, and returned. It is used primarily in Europe for chronic inflammatory conditions, environmental toxicity, post-viral syndromes, and cardiovascular risk reduction.
As of this writing, inuspheresis is not available as a standard clinical offering in the United States. Proxima Health, an Austin-based company, has signaled interest in bringing the technology to the American market, but it has not yet arrived. Patients searching for inuspheresis in California or elsewhere in the US will not currently find it here.
If you are seeking this category of treatment in the United States, therapeutic plasma exchange — performed at centers like Global Apheresis — is the established, FDA-cleared option with the deepest clinical and research foundation.
Not available in the US
Inuspheresis is currently a European procedure. Patients in the United States seeking plasma-based blood purification therapy should ask their physician about therapeutic plasma exchange, which is FDA-cleared and widely available at specialized centers.
How Does TPE Work?
To understand what makes inuspheresis different, it helps to first understand how therapeutic plasma exchange is performed.
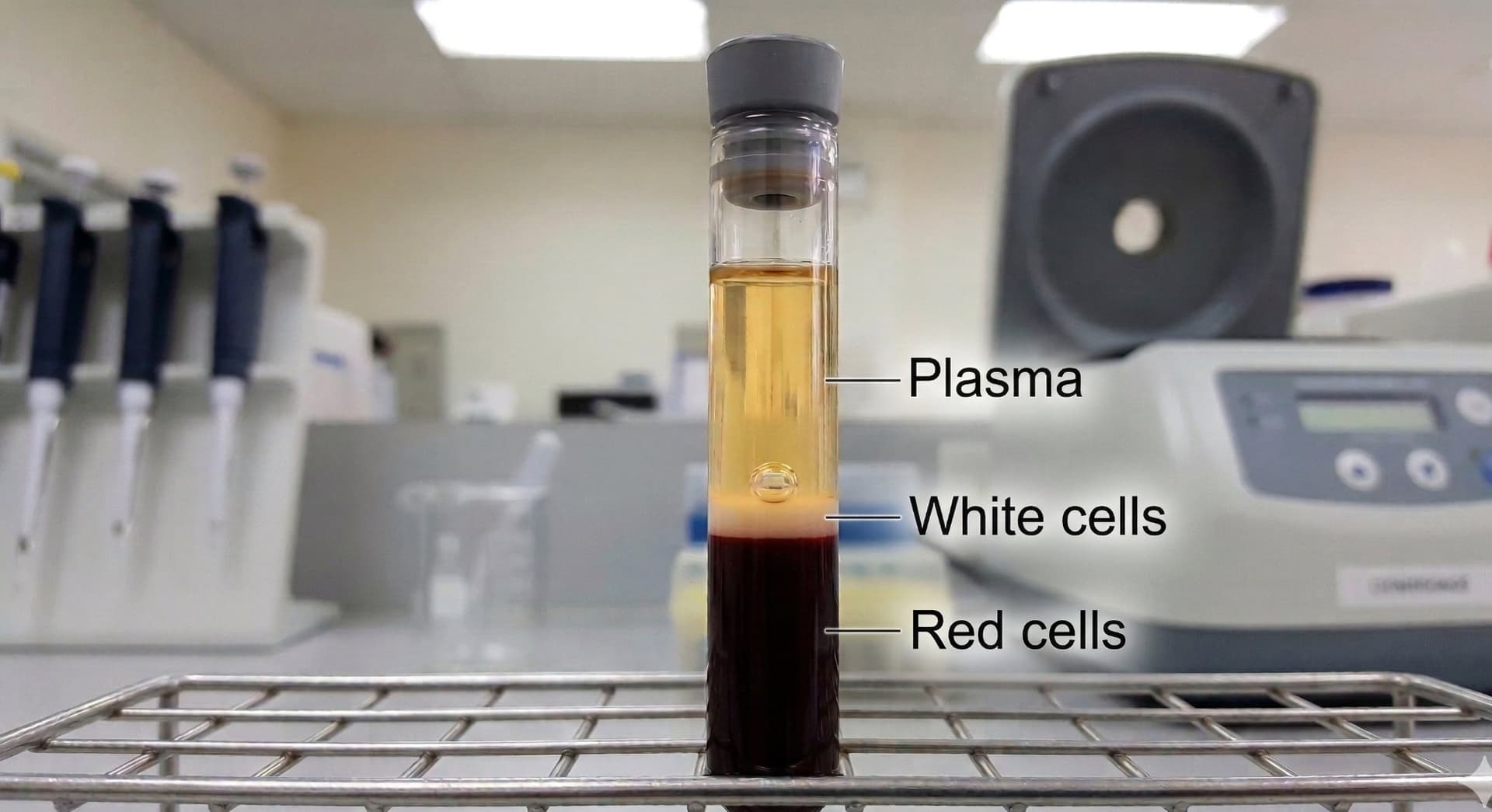
There are two distinct technologies used in plasmapheresis. The first — and the standard in the United States — is centrifugal. In this method, blood is drawn into the machine and enters a spinning centrifuge, which separates its components by density. Red blood cells, being the most dense, settle to the bottom. White blood cells collect in the middle. Plasma rises to the top. The machine then selectively removes the plasma, which is discarded and replaced with a therapeutic fluid. At Global Apheresis, this is always albumin; in hospital settings, fresh frozen plasma is sometimes used instead. There is no filter involved in this process.
The second technology is membrane filtration. A first filter physically separates plasma from the cellular components of blood. In standard single-filtration plasmapheresis using this approach, the plasma is then discarded and replaced — functionally similar to centrifugal TPE in its outcome, if not its mechanism.
How Does Inuspheresis Work?
DFPP builds on the filtration-based approach by adding a second filter. After the plasma is separated from the blood cells, it passes through a fractionator: a secondary membrane with a specific pore size. This fractionator is calibrated to trap large molecules while allowing smaller ones, including albumin, to pass through and be returned to the patient. Because most of the patient's own albumin is preserved, replacement fluid is generally not required.
Inuspheresis uses proprietary secondary filters — primarily the TKM58 and INUS 30 — designed to target different molecular profiles. The TKM58 is oriented toward broad environmental detoxification: autoantibodies, inflammatory mediators, and protein-bound toxins. The INUS 30 targets lipoproteins and is used for cardiovascular applications, removing large fractions of LDL and fibrinogen to reduce blood viscosity.
The Case for Selectivity — and Its Limits
The appeal of DFPP and inuspheresis is intuitive: why remove everything when you can target just the bad actors? Preserving the patient's own albumin reduces the need for replacement fluids, lowers costs, and avoids potential infusion reactions.
This logic holds in certain narrow indications — particularly lipid apheresis for familial hypercholesterolemia, where the target is well-defined and the filter can be calibrated precisely to catch it.
But it breaks down in the settings where most patients seeking inuspheresis are coming from: aging, Long COVID, autoimmune disease, and chronic systemic inflammation.
We Don't Know All the Molecules We Need to Remove
This is the central clinical and scientific issue with selective filtration in the context of aging and systemic disease — and it's one the research community is only beginning to grapple with.
We know that plasma contains pro-aging, pro-inflammatory factors that accumulate over time and drive biological aging. Some of these have been identified: certain inflammatory cytokines, immune complexes, dysfunctional proteins. But the full catalog is unknown. We know these factors exist and that they matter not because we've mapped all of them, but because when we remove plasma broadly and replace it — without knowing exactly what we removed — patients benefit.
This is precisely what the 2022 GeroScience study by Kim et al., co-authored by Dr. Kiprov, demonstrated. Old plasma dilution reduced measurable biological age. The 2025 Aging Cell study by Fuentealba et al. extended this finding using 35 epigenetic clocks, showing that TPE combined with IVIG produced an average reduction in biological age of approximately 2.61 years. These benefits emerged from broad, non-selective removal — not from targeting specific known molecules.
A selective filter can only remove what its pore size and membrane chemistry are designed to catch. If the molecule driving a patient's inflammatory burden or accelerating their aging process is not the right size, not the right charge, or simply not yet identified, it passes through. The filter doesn't know what it's missing. Neither do we.
TPE doesn't have this problem. It removes plasma comprehensively. Whatever is pathogenic — known or unknown, characterized or not — is cleared. The therapeutic benefit is not contingent on our current understanding of which proteins are responsible.